The muscles of the thumb of the hand recover from injury quite quickly - within one to two weeks. However, with sufficiently serious and / or chronic injuries of the thumb, damage to the structure of its tendons is often observed. Tendons are practically avascular structures, their blood supply is minimal. They recover from damage about six times slower than muscles. In addition, it is quite difficult to limit the mobility of the thumb during daily activities in order to allow damaged tendons to fully recover and prevent their re-injury.
That is why in the process of recovery after such injuries, the correct approach to therapy is extremely important. The sooner treatment begins, the faster recovery occurs. My first recommendation is not to start therapy immediately after an injury. You should wait at least 3-4 days to allow the scar tissue to fully form, and then you can apply techniques that include friction (friction massage). During the first few days after injury, you can resort to a light and shallow massage - this will help relieve pain and inflammation.
FRICTION APPLICATION
Based on my experience, I can confidently say that the most effective in the treatment of injuries of the tendons of the thumb demonstrate techniques that include friction. You can use your thumb or middle and index fingers to apply frictions. It is best to change your fingers frequently so as not to injure yourself.
Remember that pressure should only be applied in one direction. After you have worked the tendon with frictions in one direction, change the direction of the frictions to the opposite. This will help you avoid fatigue, ensure that all tendon fibers are evenly affected, and reduce the likelihood of discomfort for the client.
Work the tendon fibers in one direction for 4-5 minutes, rest a bit and start working in the other direction - in total you should spend about 8-10 minutes on this.
As the client's condition improves, the duration of therapy can be reduced. After applying the friction massage, you can gently stretch your thumb, hand and forearm.
DETERMINATION OF THE DAMAGED AREA AND THERAPY OF INJURIES OF THE TENDONS OF THE LONG AND SHORT EXTENDERS OF THE THUMB
Determining the damaged area of the tendon of the long or short extensor thumb is a very simple matter. Ask the client to extend the thumb so that the entire structure is in tension. Then apply frictional strokes of low or medium intensity across the fibers of the tendon of the short or long extensor of the thumb (depending on the nature and location of the injury). Do this at various points along the tendon to pinpoint the location of the damaged fibers. Since pain in these injuries does not radiate to nearby structures, the location of damaged fibers can be easily determined by the localization of pain sensations.
Once you have determined which part of the tendon is damaged, ask the client to relax the finger and then proceed with the friction massage. Each stroke should completely cross the damaged area.
This approach is applicable in the treatment of any tendon injury. Remember that it is necessary to determine the location of the damaged area quickly enough - with tendon injuries, prolonged stress
contraindicated.
DETERMINATION OF THE DAMAGED AREA AND THERAPY OF INJURIES OF THE SHORT AND LONG FLEXOR TENDONS OF THE THUMB
The tendons of the long and short flexors of the thumb are not so easily amenable to therapy, and it is also quite difficult to determine the damaged area. We will focus on the flexor hallucis longus tendon, as this tendon is the most commonly injured.
With one hand, hold the pad of the thumb as shown in the picture and ask the client to try to bend the finger. With the other hand, palpate the damaged tendon, located in the middle part of the eminence of the thumb (closer to the index finger) along its length, until you find the localization of pain. The client must hold the finger in tension for a while to give you the opportunity to find the damaged area. Once you have identified the damaged part of the tendon, the client can relax the finger. Perform friction at an angle of 90 degrees to the tendon fibers for 4-5 minutes, rest and repeat this action. The total duration of therapy should be 8-10 minutes, excluding one or two breaks.
DETERMINATION OF THE DAMAGED AREA AND THERAPY OF INJURIES OF THE TENDONS OF THE LONG AND SHORT MUSCLE THAT REDUCE THE THUMB
With injuries of the muscles that remove the thumb, the tendon of the long muscle that removes the thumb of the hand, located immediately behind the tendon of the short extensor thumb, most often suffers. That is why we will focus on this particular tendon.
Have the client abduct the thumb to locate the tendon. It is located slightly anterior and posterior to the extensor pollicis brevis tendon. Have the client move their thumb from side to side so that you can separate the abductor pollicis longus tendon and the extensor pollicis brevis tendon. They are located very close, therefore, in order to find the tendon of the abductor muscle, a little effort should be applied. Once you have located the tendon, palpate it to pinpoint the damaged area or areas. The main symptom of damage is local pain. Once you have located the damaged areas, ask the client to relax the thumb and proceed with therapy.
DETERMINATION OF THE DAMAGED AREA AND THERAPY OF INJURIES OF THE TENDONS OF THE ADDUCTIVE THUMB MUSCLE
Place your thumb on the medial interphalangeal joint of the thumb, and ask the client to bring the finger to the other fingers.
Use your thumb or other fingers of the other hand to palpate distally and proximal to the interphalangeal joint. Palpate the tendon fibers to locate areas of pain, then ask the client to relax the finger and get to work. As the client's condition improves, include strengthening exercises that the client can do at home. If these exercises cause pain or discomfort, then it is not time to move on to this phase of therapy. Wait at least another week. Start with simple isometric exercises like the ones I'll describe below.
EXERCISES FOR THE CLIENT
I will describe these exercises using only one hand as an example. Have the client place the pad of their index finger on the thumbnail and then try to straighten the thumb, holding it in tension for a few seconds. Then ask the client to place the top of the index finger under the ball of the thumb and then try to bend the thumb while holding it in tension for a few seconds. After this, the client should place the tip of the index finger on the medial part of the thumb between its tip and the first joint, and then try to bring the thumb to the other fingers. Then the client should place the tip of the index finger on the side of the thumb and try to move it to the side.
These exercises allow you to train your thumb in four planes without using any additional sports accessories. I recommend repeating these isometric exercises for 5 sets 4-5 times throughout the day. I believe that this is the most affordable and effective way to strengthen the muscles and tendons of the thumb.
Dr. Ben E. Benjamin
Source: www.massage.ru
Anatomy
The long extensor of the fingers refers to the muscles of the lower leg, or rather, to its anterior group. It is located outside of the anterior tibial muscle. The muscle goes down, turning into a narrow tendon, which is amazingly strong. Further, it diverges into 4 beams: each is designed for a separate finger. It is attached at the level of the proximal phalanx. At the point of attachment, the beam diverges into 3 small parts, which make it possible to set in motion any part of the foot.
The mobility of the thumb is carried out by the work of several muscles at the same time. This complex structure is necessary, as it is he who helps to maintain balance and the ability to walk upright. The long flexor of the big toe is a muscle that belongs to the posterior group of the lower leg. Its growth begins in the region of the lower 2/3 of the fibula. It goes down the limb to the sole and turns into a tendon. On the foot, it grows a little into the tendon responsible for the movements of the remaining fingers. So it turns out that the movements of all phalanges depend to one degree or another on his work. It is fixed on the nail phalanx.
Muscles responsible for flexion and extension of the fingers
The extensor muscles in the lower extremities are appropriately named and do heavy work on a daily basis during movement. These include:
- tibialis anterior,
- long extensor,
- thumb extensor.
The calf extensors are very strong and important for the ability to walk straight.
bending
The long flexor makes it possible during movement (when a person is walking or running) to push off the floor in the right way. He also participates in the supination of the foot - the ability to stand on the toe and maintain balance.
The long flexor of the thumb is named for its functions: it helps to bend it, and can also affect the entire metatarsus due to the features of its structure. Like other muscles of the lower leg, it is involved in the work of the foot, helping it to bend, as well as adducting and supinating. Also, the presence of this tendon makes the longitudinal arch of the foot stronger.
Extension
The long extensor is included in the group of muscles of the lower leg, located in front, closer to the inside. In addition to its direct purpose, this tendon extends the foot. To do this, it works together with the 3rd peroneal muscle. In the case of rigid fixation of the foot, it will bring the lower leg closer to it.
The long extensor of the thumb is responsible for the ability to straighten the big toe, and also sets the foot in motion, raising its front edge.
Muscle performance tests
The calf extensors can lose their strength due to a number of reasons. You can check its condition and performance using simple tests that the doctor conducts during the examination:
- With one hand, you need to hold the metatarsus in the usual position, and with the other, gently but firmly bend your toes. A person should strive to straighten them. If he succeeds, the highest mark is 4 or 5.
- The person lies on his back, a soft roller is placed under his knees. The metatarsus is held by force. At the same time, he should try to straighten his fingers. If he succeeds, the highest mark is 3.
- The position is the same. The doctor feels the tendon, while the person should try to straighten his fingers. If he succeeds, the highest mark is 1.
In a normal state, a person receives 5 points. The strength may decrease if the tissues do not receive sufficient nutrition, or if innervation has occurred.
Causes of muscle dysfunction
The foot extensors can lose strength or suffer other damaging effects for a number of reasons:
- atrophy with age due to disruption of tissue nutrition,
- pathologies in the work of the endocrine system,
- connective tissue diseases,
- fermentopathy,
- polyneuritis,
- complications after injury
- too much physical activity.
The main cause of the lesion is tendinitis. This is an inflammatory disease of the tendons that can also affect nearby muscle tissue. Dystrophic destruction can become chronic, which is very dangerous and almost incurable.
Also, pain in the foot can occur due to the deposition of salts and the formation of growths on the bone tissue. The reason for this may be the use of certain drugs, etc.
Diagnostics
The extensor hallucis longus or the entire metatarsus may be damaged. On examination, the doctor notes "spanking" when walking or dragging. The doctor performs palpation, as well as a series of tests that help assess the nature of the damage. If muscles have been damaged, weakness and soreness may occur when exercising with or without resistance. If there is weakness of the entire metatarsus, including the little finger, compression of the nerve is possible.
The foot remains mobile due to the presence of various types of muscles in its structure, including the short extensor of the big toe. Short muscles are those muscles that do not go beyond the area of \u200b\u200bthe foot. The long ones are based at the ankle and attached to the foot. The most important function of these muscles is considered to be the flexion and extension of all fingers and the movement of the phalanges located on the feet.
Muscles localized in the toes are responsible for performing the correct movements of the bone levers in the ankle joint, and if they are damaged, the functioning of this entire department is disrupted. In the structure of the foot there are short and long muscles. There are also several flexors of the fingers: a short flexor of the foot of the little finger and other fingers. Foot mobility is provided by two extensor tendons.
short muscles
The extensor digitorum brevis is a muscle that looks like a wide, flat band that runs along the outside of the foot. It is attached to the heel bone, from where it moves to the fingers and there it is already transformed into three tendons. At the very top, they connect with other tendons, and then attach to the phalanges. The muscle is nourished with useful substances by the bloodstream, which moves along the tibial artery, and the supply of nerve sensitivity to these tissues is provided by the peroneal nerve.
long muscles
The long extensor of the big toes is attached to the tibia at one end and to the phalanges at the other. Its main function: flexes the thumb, unbends it. The extensor unites with the so-called square muscle and is divided into four tendons. All these tendons are attached to the four phalanges on the lower extremities, which allows you to bend and unbend the foot and move it in different directions. foot is located on the side of the lower leg on its outer side and is attached to the tibia. Further, it passes through the region of the lower leg and, penetrating the structure of the foot, is divided into five processes that are attached to the phalanges. This structure is responsible for the extension and flexion of the lower limb, its supination and is responsible for rotational movements.
Diseases and injuries of the long extensor are dangerous because they severely limit the mobility of the injured limb. For example, with tendonitis of the long extensor tendon, it becomes impossible to bend and straighten the fingers, the gait is disturbed, such a condition without proper treatment can lead to disability.
Strengthening the feet with exercise therapy
The extensor of the big toe can be strengthened so that it is not damaged by excessive stress or various diseases. For this, various physical therapeutic exercises are performed. Such measures are considered an excellent prevention of leg pain.

There is such a term as the core of the legs, which means the totality of all the small muscles and tendons that stabilize the body during activity and movement. The function of these fabrics is to reduce and absorb the impact of walking while maintaining balance throughout the body. When these muscles are weakened, physical activity passes to the plantar fascia, in which pathological processes develop due to overstrain. The weakening of the ligamentous apparatus over time provokes a change in gait and becomes the root cause of pathologies in the knee and hip joints, and also causes disorders in the spine.
To strengthen the tendons and muscles of the foot, it is necessary to perform therapeutic exercises several times a week. The advantage of such physical education is that anyone can perform it at home. Below are some of the exercises that help strengthen the ligamentous apparatus on the legs.
- You should take a towel with your toes and stretch it around the room for several meters. Next, form a lump from this towel with your fingers. Grab the towel again and move it in the opposite direction. Repeat using the other lower limb.
- Scatter small objects on the floor - buttons, medium-sized balls and sit on a chair. Now try to collect these items of the feet in some kind of box. Repeat with the other leg.
- The first few times this exercise is carried out in a sitting position, then standing. You should put your foot on the floor, then pull your fingers towards you and at the same time you need to form an arc with your feet.
- Sit on the floor, legs extended forward in a straight position. Now you need to tighten the foot and stretch it in such a way as if you were standing on heels. Fix the position and try to slowly turn the foot towards you. Repeat several times.
A noticeable result can be noted after a few months of regular classes. The muscles are gradually strengthened, the arch of the foot rises. Blood circulation improves, the sensitivity of the foot increases, the stability of the whole organism is restored.
The long flexor thumb is located deep under the calf and soleus muscles and
covers the posterior tibial muscle. The muscle is located laterally on the back surface
shins. The belly muscle attaches to the posterior surface of the fibula, joining the tibialis posterior and flexor digitorum longus just behind the medial malleolus.
These muscles pass through the tarsal canal, formed by the medial surface of the calcaneus and the fibrous plate of the flexor tendon retinaculum. In structure and function, this structure is identical to the carpal tunnel. The tibial artery and tibial nerve also pass through the tarsal canal.
The flexor hallucis longus, flexor digitorum longus, and tibialis posterior produce inversion of the foot and plantarflexion of the ankle. In addition, the flexor thumb longus flexes the thumb at the metatarsophalangeal and interphalangeal joints. This movement is necessary in the take-off phase of walking for efficient energy transfer. The center of gravity shifts from the heel through the foot to the big toe at the end of the stance phase and the energy generated by the hips, knees and shins passes through the foot and big toe, moving the human body forward.
The flexor hallucis longus plays a significant role in directing this energy. In addition, the long flexor of the big toe is involved in providing dynamic stabilization of the medial arch of the foot. Together with other muscles passing through the tarsal canal and the muscles of the foot, the flexor hallucis longus controls the pronation of the foot during walking, running and jumping. The long flexor of the big toe provides effective grip of the foot with the surface and helps us to effectively maintain balance when walking.
Problems with this muscle can flatten the medial arch of the foot and destabilize the ankle, resulting in pain, loss of sensation, and gait disturbance when walking.
Palpation of the long flexor of the big toe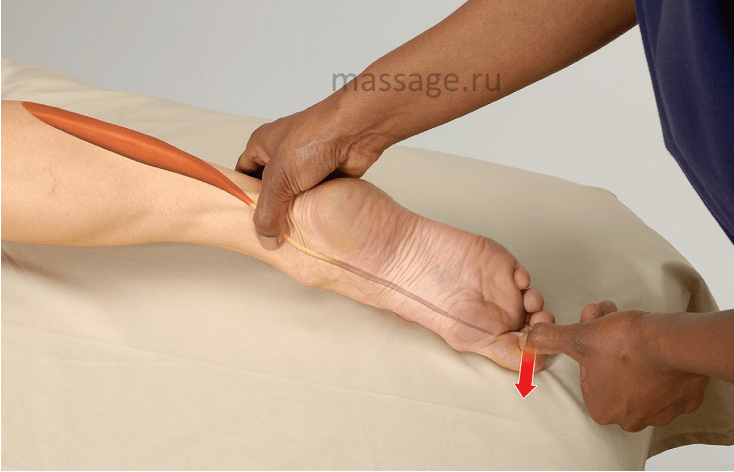
The client lies on his stomach
1. Standing at the client's feet, use your thumb to locate the medial malleolus.
2. In a smooth sliding motion, slide your thumb into the space between your ankle and Achilles tendon. (Caution: the tibial artery and nerve also pass through this area. Move your finger if the client feels tingling and numb, and if you feel a pulse.)
3. There are three tendons in this area. Palpate the tendon located most
is the tendon of the long flexor of the big toe.
4. Ask the client to bend their thumb to make sure you did everything right.
CLIENT EXERCISE: SEATED TOE STRETCH
1. Sit on the floor with your feet straight in front of you.
2. With your knees relaxed, bend at the waist and lean forward.
3. Take the big toe with your fingers.
4. Gently pull your thumb back towards your knee for 5-10 seconds, then release.
This exercise can be done with all toes.
Injury to extensor hallucis longus within the terminal phalanx. This damage does not differ from similar damage to the extensor of the remaining fingers. In the presence of damage localized proximal to the main joint, there are conditions for applying a primary tendon suture, however, after 3-4 weeks, a secondary tendon suture is not feasible due to the reduction of the ends of the tendon.
To fix a defect free tendon graft required or better to apply tendon transposition. During transposition, the tendon of the common extensor of the second finger is used, to which the distal end of the extensor tendon of the thumb is sutured.
extensor longus tear occurs quite frequently. This damage is divided into the following types:
1. direct or indirect rupture caused by trauma;
2. spontaneous rupture:
a) professional hazards,
b) tendon changes,
c) rupture due to damage to the limb.
tendon rupture due to direct trauma and the result of his treatment by tendon transposition are shown in the figure (own observation).
"Spontaneous" tendon ruptures due to occupational hazards, were described at the end of the last century by military doctors (Zander). The left hand of the army drummers, when holding the drumstick, was in a position of pronounced dorsiflexion, due to its unnatural position, tendovaginitis developed, degeneration of the tendons, which led to a "spontaneous" rupture.
A hand injury as a result of a fall of a log in a 47-year-old bricklayer, there is no active extension of the thumb of the right hand (a).Immediately after the injury, only the skin was sutured. Transposition of the tendon of the own extensor of the index finger was performed in conditions of scar tissue. The result of the intervention is shown in photo b.
Wurtenau described 59 cases of rupture tendons the drummers of the Prussian army. These typical breaks are known in the literature as "drummer's palsy" ("Trommerlahmung" or "Drummer's palsy").
IN Literature describes tendon ruptures due to various diseases. Thus, ruptures due to suppuration, gout, syphilis, tuberculous tendovaginitis (10 cases of Mezon), gonorrhea (Melchior), polyarthritis (Lederich, Herris) and rheumatism (Wadstein).
At post-traumatic tendon rupture from the moment of injury to tendon rupture, there is a latent period lasting from several days to several years. Linder (1885) and Geinicke (1913) first drew attention to the rupture of the tendon of the long extensor of the thumb after a fracture of the radius. Mek Master in 1932 collected a total of 27 such cases from the literature.
F. Steppelmore in 1940 he wrote a generalizing report on 148 cases already known. In 1955, G. Strendell, including his own 14 observations, reports 60 new cases of these injuries. Thus, 208 cases of post-traumatic tendon rupture are known in the literature. This type of injury prevails in women in 67-37%. In most cases, ruptures occur with a dislocation or fracture of the radius without displacement of the fragments. The frequency of rupture of the tendon of the long extensor of the thumb, according to different authors, is different.
The frequency of this complications after fracture of the beam according to Gauk 6:100, according to Moore 3:500, according to Steppelmore 3:1000, according to Markus 4:2134, according to Böhler 1:500.
Long extensor thumb begins on the dorso-radial surface of the middle third of the ulna and on the interosseous membrane. Its tendon at the level of the wrist passes in a separate tendon sheath. This space, the third dorsal tendon sheath, is essentially a canal to the bone. It is deeper and narrower than the other extensor sheaths. The tendon runs obliquely and, crossing with the long and short radial extensor of the hand, forms the ulnar edge of the "anatomist's snuffbox".
extensor tendon within the proximal phalanx of the thumb, it expands and attaches to the base of the distal phalanx. The main function of the long extensor of the thumb is to extend it at the terminal, main and saddle joints. In addition, this muscle contributes to the retroposition of the thumb, is involved in dorsiflexion of the hand and, together with the adductor muscle of the thumb, in bringing the latter. Its most important function is to fix the saddle joint.
In view of the fact that the condition for good capture is fixation muscles of the centrally lying joints, the loss of the function of the long extensor of the thumb leads to an almost complete loss of the function of gripping the thumb.
overwhelming most post-traumatic tears, a long time after the moment of injury, occurs not as a result of unusual efforts, but in the process of habitual daily movements. Tendon rupture in these cases is not accompanied by pain. After a rupture, the thumb hangs down, the distal phalanx assumes a bent position and cannot be actively extended. Retroposition and adduction of the thumb may not be feasible. The contours of the ulnar edge of the "anatomical snuffbox" are smoothed out.
In view of the lack stabilization of the saddle joint the grip is not strong enough, so the patient is unable to use scissors, write, or do up buttons.
Usually gap localized at the level of the distal edge of the dorsal transverse carpal ligament. Above this level, rupture is rare, occurring in about 7% of cases. The distal end of the tendon is felt over the first metacarpal bone in the form of a knot. The proximal end of the tendon contracts and moves quite far in the central direction. The tendon sheath collapses.
In a relationship pathogenesis of long extensor tendon rupture thumb, the opinions of the authors agree. Emphasis is placed on the special role of the canal and the course of the tendon. Levy and Cohen consider Lister's tubercle, which forms the radial edge of the canal, as a hypomochlion, over which the tendon elongates and deflates during movement.
The value of fractures of the radius for subcutaneous rupture of the extensor thumb has been studied by many authors. According to most researchers, the callus formed after a fracture of the radius narrows the tendon canal, and the existing bone fragments, gradually damaging the tendon, can contribute to its rupture.
According to Rau And Weigel, in tendon rupture, deterioration of tendon vascularization at the age of over 25-30 years is of decisive importance, since in adults there are no longitudinal intratendinous vessels, and the external vascular network may suffer from various types of injuries. Strendell believes that the occurrence of a post-traumatic rupture of the tendon is associated with a violation of its blood supply due to trauma (hematoma, thrombosis, degenerative changes in the connective tissue), and the rupture occurs at the point of least resistance, that is, within the vagina.
Complete transection of the tendon with a sharp bone fragment is considered only in rare cases.
Treatment of post-traumatic rupture of the tendon of the long extensor of the thumb must always be operational. According to their principle, operations are divided into two groups, namely: methods of direct connection of the ends of the tendon and methods of tendon transposition - connection of the distal end of the torn tendon with another adjacent extensor tendon.
Method of direct joints of tendon ends, due to stump reduction and tendon degeneration, is now rarely used. Methods for replacing tendon defects also did not lead to satisfactory results (free tendon grafting, replacement of the defect with fascia or artificial material, etc.).
Currently dominated tendon transposition method. This method was first applied by Duplay (1876). He attached the distal end of the long extensor of the thumb to the long radial extensor of the hand. The extensor tendons that can be used in transposition are shown in the table.
For transpositions As a rule, it is best to use a tendon whose direction of pull and amplitude of sliding does not differ from the tendon-muscle motor being replaced. When considering the extensor tendon from these two points of view, it turns out that the requirements are best met, first, by the tendon of the extensor extensor of the index finger, and secondly, by the tendon of the long radial extensor of the hand.
The first of these was first used for this purpose by Mensch (1925), and in the recent past its use has been recommended by many authors (Bunnell, Pulwertaft, Christoph) and especially J. Böhler. The advantage of the long radial extensor is its anatomical proximity to the rupture site and the fact that the direction of its thrust acts from the ulnar side. Given its anatomical location, the tendon is recommended for transposition by Schlatter and Fett. The disadvantage of this tendon is that it has less movement than the extensor pollicis longus tendon.
Transposition of the tendon of the own extensor of the index finger Strendell performs as follows: the tendon of the own extensor of the index finger is crossed over the head of the II metacarpal bone through a transverse skin incision of 1 - 2 cm. The distal end of the tendon is attached to the tendon of the common extensor of the index finger so that when the finger is straightened, it resists the rotation of the index finger. Within the wrist, according to the location of the tendon, a longitudinal skin incision is made, through which the cut tendon of the own extensor of the index finger is removed.
Then, using new cut at the level of the middle of the I metacarpal bone, the stump of the tendon of the long extensor of the thumb is released, and then it is connected "end to end" with the tendon of the own extensor of the index finger, held under the skin.
 Rupture of the tendon of the long extensor of the thumb due to a fracture of the radius
Rupture of the tendon of the long extensor of the thumb due to a fracture of the radius
Case of own observation: B. I., a 28-year-old teacher, received a fracture of the radius in a typical place with a slight displacement of the fragments. After reposition, four weeks of fixation, and three weeks of functional therapy following the removal of the plaster cast (Fig. a), the patient felt healthy. However, on the eighth week, while cleaning the apartment, in the absence of any strong movements, the patient felt a crunch in her thumb, after which it became impossible to straighten it. The position of the thumb, typical for a rupture of the extensor tendon, is shown in Fig. b.
In terms of location, action and number, the muscles of the toes are almost similar to the muscles of the fingers of the hand, but, as already indicated, depending on the little developed activity of the toes, the muscles of the rear of the foot are more related to movement in the ankle joint, and the muscles of the plantar side are involved in strengthening the arch of the foot.
Extensors and flexors of the toes
Between the extensors of the fingers (dorsal flexors) and their flexors (plantar flexors) we find long and short extensors, as well as long and short flexors. The first are located on the front surface of the lower leg and on the rear of the foot, the second - on the back surface of the lower leg and on the sole.
Among the extensors we have the extensor digitorum longus and the extensor hallucis longus, which have already been described above; it remains for us to disassemble only the short extensors of the fingers.
Short finger extensor(m. extensor digitorum brevis, Fig. 72-11) begins on the dorsum of the calcaneus; its innermost part stands out under the name of the short extensor of the thumb (m. extensor hallucis brevis, Fig. 72-22). At the level of the metatarsal bones, the muscle fibers pass into the tendons of the first four fingers. All of them obliquely fit (outside inwards) to the outer side of the tendons of the long extensor and merge with them at the base of the first phalanx, except for the tendons of the thumb. The tendon of the short extensor of the thumb is attached directly to the first phalanx.
The short extensor of the fingers mainly acts on the first phalanges. The oblique arrangement of its tendons allows the abduction of the fingers outward in the metatarsophalangeal joint. Acting simultaneously with the long extensor of the fingers, the short extensor produces pure extension of the fingers at the metatarsophalangeal joint. The tendon of the short extensor of the first finger, attaching directly to the first phalanx, produces its extension.
Innervation: deep peroneal nerve (n. peroneus profundus, L IV-V and S I).
Among the flexors of the fingers, there are: a long flexor of the thumb and a common long flexor of the fingers with an additional head starting from the calcaneus, a square muscle of the sole and a short common flexor of the fingers. In addition, there is a short flexor for both the thumb and little finger.
flexor digitorum longus(m. flexor digitorum communis longus, Fig. 66-7) is located in the deepest layer of the lower leg. It originates from two-thirds of the posterior surface of the tibia, in addition, part of its fibers originate from the tendon arch formed by the fascia of the tibia.
Thus, the beginning of its muscle fibers reaches the fibula. The posterior tibial muscle, approaching the formed tendon of the long flexor, crosses it and is located directly near the inner ankle. The tendon of the long flexor of the fingers, going down, is located closer to the midline of the lower leg and passes to the sole. On the sole, it receives a tendon stalk from the long flexor of the thumb and, in addition, a short additional head is attached to it from the lower and inner surface of the calcaneus - square muscle of the sole(m. quadratus plantae, s. sago quadrata Sylvii, Fig. 66-23). Then, at the level of the base of the metatarsal bones, the common tendon of the long common flexor of the fingers splits into four bundles, which immediately give rise to the so-called vermiform muscles, leaving from the inside (from the side of the first finger) side of its tendons. Moving further forward, each tendon of the common long flexor lies in a canal formed by the bifurcation of the corresponding tendon of the short flexor, just as it was on the hand of the superficial and deep flexors of the fingers. Located together with the short common flexor "of the fingers in the bone-fibrous sheath of the fingers, the tendons of the long flexor end, attaching to the third (nail) phalanges of the fingers -
The long common flexor of the fingers flexes the third phalanges over the second and the second over the first; at the maximum of its contraction, it can somewhat bend the first phalanx over the metatarsal bone; in addition, it informs the IV and V fingers of some deviation inward, which is especially evident in the position of their nail phalanges. This last action is explained by the oblique (inside outward) direction of the tendons of the IV and V fingers on the sole. If the action of its accessory head and the action of the short common finger flexor are added to the action of the general long flexor of the fingers, then this deviation is destroyed.
Duchenne and Poirier completely deny the action of the long common flexor of the fingers on the ankle joint during the upper support. Braus, on the other hand, believes that with the upper support, the common long flexor of the fingers can produce plantar flexion, supination (turning the sole inside) and abduction medially (from the midline of the foot), with supination most pronounced, plantar flexion the least, and abduction medially corresponds to the action posterior tibial muscle. When a person is in a standing position, the long flexor of the fingers strengthens the arches of the foot and can extend the lower leg (plantar flexion) when lifting the torso on toes.
Innervation: tibial nerve (n. tibialis, L V and S I).
Short common finger flexor(m. flexor digitorum communis brevis, Fig. 74) starts from the lower surface of the calcaneal tuber, from the posterior third of the upper surface of the plantar aponeurosis and from the intermuscular septa. At the level of the base of the metatarsal bones, it forms four tendons, which split longitudinally at the level of the first phalanges and, having passed the corresponding tendons of the long
the common flexor of the fingers, pass through the bone-fibrous sheath and are attached to the sides of the second phalanges, reaching their articulations with the third. Their attitude and construction are quite consistent with the attitude and construction of the superficial and deep flexor of the fingers, which were described above. The tendon of the flexor of the fifth finger is sometimes very thin and is not pierced by the tendon of the common long flexor of the fingers, sometimes it is completely absent.
The short common flexor of the fingers flexes the second (phalanges) and almost does not show 4 its action on either the first or third phalanges. With a lower support, its main action is to strengthen the longitudinal arch of the foot (Fig. 74) and plantar aponeurosis.
Innervation: plantar internal nerve (n. plan-taris medialis, L V and S I).
flexor thumb longus(m. flexor hallucis longus, Fig. 66-19, 15) is the outermost muscle of the deep posterior muscle layer of the lower leg; it begins on the middle lower third of the posterior surface of the fibula; going down and inside, it passes into the tendon, located in the groove located on the posterior surface of the talus, fits under the internal process of the calcaneus (sustentaculum tali) and goes to the inner edge of the foot.
On this path, the tendon of the long flexor of the thumb crosses with the tendon of the long common flexor of the fingers, connects to it with a tendon bundle and then, passing between both parts of the short flexor of the thumb and both sesamoid bones of the metacarpophalangeal joint of the thumb, reaches its nail phalanx, where it attached (Fig. 74-4).
The long flexor thumb strongly flexes the second phalanx and has little effect on the metatarsophalangeal joint. Duchenne completely rejects its influence on the ankle joint. According to Braus, the flexor hallucis longus plays a large role in pushing the foot off the ground. It is also necessary to note its importance in relation to the movements of the entire foot. It is predominantly a plantar flexor, but at the same time, with the upper support, it abducts the foot inwards and supinates it. With lower support, the long flexor of the big toe strengthens the arch of the foot in the longitudinal direction and counteracts the formation of a flat sole (pes planum).
Innervation: tibial nerve (n. tibialis, L V and S I-II).
Flexor thumb short(m. flexor hallucis brevis, Fig. 74-2; 75-1) is divided into two parts. Both parts of it start from the sphenoid bones, from the ligamentous apparatus connecting the plantar surface of the calcaneus and metatarsal bones, and from the plantar aponeurosis. Heading towards the thumb along the metacarpal bone, the short flexor of the thumb is divided into two parts and attached to the tubercle of the first phalanx: one on the outside, the other on the inside. Both tendons have sesamoid ossicles.

Rice. 75. Deep muscles of the foot. (Poirier.) 1 - short flexor of the thumb, 2 - transverse head of the adductor thumb muscle, 2 "- oblique head of adductor muscle of the thumb, 3 - short flexor of the V finger, 4 - muscle opposing the V finger, 5 - tendon of the long peroneal muscle - its course along the plantar surface and attachment
The short flexor thumb flexes the thumb at the metatarsophalangeal joint, which is especially important when standing on toes. Acting with separate heads, the short flexor of the thumb can abduct the first phalanx to one side and the other (from the midline of the foot). Starting from the deep ligamentous apparatus of the foot and to the side of the plantar aponeurosis, it strengthens the internal longitudinal arch of the foot along with other muscles.
Fifth finger flexor short(m. flexor digiti quinti, Fig. 75-3) starts from the fibrous sheath of the long peroneal muscle, from the crest of the lower surface of the cuboid bone, from the base of the metatarsal bone of the fifth finger and is attached to the base of the first phalanx of the fifth finger. It flexes the V finger at the metatarsophalangeal joint, and also strengthens the outer longitudinal arch of the foot through the plantar aponeurosis.
Innervation: external plantar nerve (n. plantaris lateralis, S I-II).
Muscles that abduct the toes to kick three and outward from the midline of the foot
Abduction, which is possible in the metatarsophalangeal joints, is performed in the same way as on the hand, by means of the interosseous and vermiform muscles, and in the thumb and small fingers, also by specially abducting muscles. Only the opposing muscle of the thumb is missing here; as for the same muscle of the fifth finger, it is sometimes observed. On the foot, as well as on the hand, in this group there should be 10 abductor and adductor muscles. Of these, the muscles that abduct and adduct the thumb, as well as the abductor of the thumb, are located on the sole, and the rest are between the metatarsal bones, which is why they, like the muscles of the hand, are called interosseous. The vermiform muscles, which were mentioned in the description of the long common flexor of the fingers, being located on the inside of its tendons, also take part in the abduction of the II finger and the adduction of the III, IV and V fingers.
On the foot, the middle line, towards which adduction (adductio) will be performed and away from which abduction (abductio) will be performed, coincides with the middle line of the second finger. Thus, only the second finger will have two interosseous muscles that abduct to both sides of the midline, while the remaining fingers will have interosseous muscles that abduct from the midline and lead to it.
At the thumb, we have an independent muscle that abducts the thumb and an independent adductor.
Abductor thumb muscle(m. abductor hallucis, Fig. 74-3) lies superficially under the fascia on the inner edge of the foot and forms an elevation of the thumb. The abductor muscle starts directly from the lower part of the inner surface of the calcaneal tuberosity, as well as from the ligamentous apparatus of the foot and plantar aponeurosis; it is attached by a well-developed tendon to the inner edge of the first phalanx, fusing with the tendon of the inner head of the short flexor of the thumb. Sometimes the abductor thumb muscle sends a tendon extension to the extensor tendon of the thumb. It produces the abduction of the thumb from the midline of the foot, in which it is partly helped by the inner head of the short flexor of the thumb.
The muscle that abducts the thumb can be attributed to a static type: pinnate arrangement of fibers (powerful tendon). Its main value is to strengthen the inner arch of the foot. Abduction of the thumb is weakly expressed.
Innervation: internal plantar nerve (n. plantaris medialis, L V and S I).
adductor thumb muscle(m. adductor hallucis, Fig. 75-2, 2 ") consists of two heads. One of them, obliquely located, starts from the cuboid bone, from the third sphenoid, second and third metatarsal bones, and also from the fibrous sheath of the long peroneal muscle and goes obliquely from the middle of the foot to the first finger.The second head, transversely located, starts from the head of the metatarsal bone of the fourth finger and, on the way to the first finger, crosses the heads of all other metacarpal bones in the transverse direction, receiving separate muscle bundles from them and from the intermetatarsal ligaments.
The obliquely located head, approaching the first finger, fuses with the outer head of the short flexor of the thumb and together with it will bring the thumb to the midline of the foot. The transversely located head of the adductor thumb muscle is more independent than was observed on the hand, and some (Lebuk) even indicate that this muscle has an independent attachment on the first phalanx: on the one hand, it sends a continuation to the rear of the thumb to its extensor , on the other hand, part of the fibers, passing through the attachment of the oblique head of the adductor muscle of the thumb and its short flexor, ends at the bone-fibrous sheath of the thumb. The oblique head has the strongest adductor effect on the first phalanx of the big toe and, as Duchene points out, is an active ligament that does not allow the heads of the metatarsal bones to diverge, and thus strengthens the transverse arch of the foot.
Innervation: internal and external plantar nerves (n. n. plantares medialis et lateralis, S I-II).
Abductor fifth finger muscle(m. abductor digiti quinti, Fig. 74-5), like the muscle that removes the thumb, is located superficially, but only on the outside. The muscle abducting the V finger begins from the lower surface of the posterior external tubercle of the calcaneus, from the inward surface of the plantar aponeurosis and from the intermuscular septum that separates it from the short flexor of the fingers. Heading forward along the metacarpal bone of the fifth finger, it ends on the outer surface of the base of the first phalanx of the fifth finger and on the lower surface of the bursal ligament of the metatarsophalangeal joint.
In most cases, the muscle that abducts the V finger is only a flexor of the first phalanx, and only in children can it still be abducted. Being located on the outside from the heel to the main phalanx of the fifth finger, it, of course, has a great influence on strengthening the outer arch.
Innervation: external plantar nerve (b. plantaris lateralis, S I-II).
The abduction and adduction of the remaining fingers is performed with the help of the interosseous muscles; they are located like the interosseous muscles of the hand, on the one hand, in the deepest layer on the sole (interosseous internal muscles), on the other hand, on the back of the foot (interosseous external muscles). As on the hand, there are three internal interosseous muscles on the foot, four on the outside; the inner ones will lead to the midline of the foot, the outer ones will lead away from the midline; you just need to remember that the midline of the foot passes through the second toe and therefore two abductors will be at the second toe, and not at the third, as we saw on the hand.
Adductor internal interosseous muscles(m. m. interossei interni, Fig. 76) start from the posterior third of the lower edge of each of the last three metacarpal bones (V, IV and III) and from the lower surface of their base. They lie more superficial than the interosseous spaces themselves, so that they completely cover the lower surface of the metacarpal bones. They end in a completely different way than the internal interosseous muscles of the hand: in most cases, they are attached only to the lateral internal (on the side of the thumb) part of the first phalanx and to the bursal ligament of its joint; they do not continue to the extensor tendon of the fingers.

According to their location and attachment, the internal interosseous muscles are the muscles leading to the midline of the foot III, IV and V fingers; the second finger has no adductor muscle, since it lies on the midline of the foot, and the big one has its own adductor, described above (Fig. 75-2).
Innervation: deep branches of the external plantar nerve (rami profundi n. plantaris lateralis, S I-II).
Abductor external interosseous muscles(m. m. interossei externi, Fig. 77) are located on the back of the foot, fulfilling all the gaps between the metacarpal bones. They are biceps and start from the lateral parts of the metacarpal bones facing each other, from the lower surface of their bases and the dorsal interosseous fascia. Starting from two opposite sides, they form pennate muscles, the tendons of which are attached to the base of the first phalanges and to the bursal ligament of the joint on the outside of the III and IV fingers and on both sides of the II finger. They do not continue to the extensor tendon of the fingers; rather, you can find continuations to the cartilaginous thickenings of the bag of the metatarsophalangeal joint.
The interosseous muscles of the IV, III and II fingers are abducting from the midline of the foot. These movements in the foot are very limited, as they are constantly constrained by shoes, and are most marked in children or people who do not wear shoes. Approaching the first phalanx from both sides, more from the plantar surface, and combining its action with the action of the internal interosseous muscles, the external interosseous muscles of the IV, III and II fingers bend the first phalanx; the same movement is produced by the abductor V finger in combination with the internal interosseous V finger.
Innervation: deep branches of the external plantar nerve (n. plantaris lateralis, S I-II).
vermiform muscles(m. m. lumbricales,) mentioned above when describing the long common flexor of the fingers, from the tendons of which they begin, also take part in the abduction of the fingers. Located on the inside of each tendon of the II, III, IV and V fingers, they are attached to the inside of the first phalanges of the same fingers, and, therefore, will contribute to the work of the interosseous muscles that produce abduction in their direction. In the second finger, they will produce abduction from the midline, and in the remaining (III, IV and V) fingers, they will lead to the midline.

The vermiform muscles, to a certain extent, can participate in the flexion of the first phalanges.
Innervation: internal plantar nerve (n. plantaris medialis); external plantar nerve (n. plantaris lateralis to the first, third and fourth, L V and S I-II).
To the muscles of the foot, one must also add a non-permanent muscle that opposes the fifth finger.
Opposite V finger muscle(m. opponens digiti quinti, Fig. 75-4). Man does not have an opposing muscle of the thumb, since the thumb, being one of the main points of support, has lost all significance for grasping. The opposing muscle of the fifth finger is important for adapting the sole to uneven ground. Even when it exists, it is poorly developed and not completely separable from the flexor brevis and abductor digit V. It differs from the muscles mentioned only in that it is attached not to the first, but to the metacarpal bone of the fifth finger. During its contraction, the muscle opposing the V finger pulls the metacarpal bone somewhat inward (toward the midline of the foot) downward.