The long flexor thumb is located deep under the calf and soleus muscles and
covers the posterior tibial muscle. The muscle is located laterally on the back surface
shins. The belly muscle attaches to the posterior surface of the fibula, joining the tibialis posterior and flexor digitorum longus just behind the medial malleolus.
These muscles pass through the tarsal canal, formed by the medial surface of the calcaneus and the fibrous plate of the flexor tendon retinaculum. In structure and function, this structure is identical to the carpal tunnel. The tibial artery and tibial nerve also pass through the tarsal canal.
The flexor hallucis longus, flexor digitorum longus, and tibialis posterior produce inversion of the foot and plantarflexion of the ankle. In addition, the flexor thumb longus flexes the thumb at the metatarsophalangeal and interphalangeal joints. This movement is necessary in the take-off phase of walking for efficient energy transfer. The center of gravity shifts from the heel through the foot to the big toe at the end of the stance phase and the energy generated by the hips, knees and shins passes through the foot and big toe, moving the human body forward.
The flexor hallucis longus plays a significant role in directing this energy. In addition, the long flexor of the big toe is involved in providing dynamic stabilization of the medial arch of the foot. Together with other muscles passing through the tarsal canal and the muscles of the foot, the flexor hallucis longus controls the pronation of the foot during walking, running and jumping. The long flexor of the big toe provides effective grip of the foot with the surface and helps us to effectively maintain balance when walking.
Problems with this muscle can flatten the medial arch of the foot and destabilize the ankle, resulting in pain, loss of sensation, and gait disturbance when walking.
Palpation of the long flexor of the big toe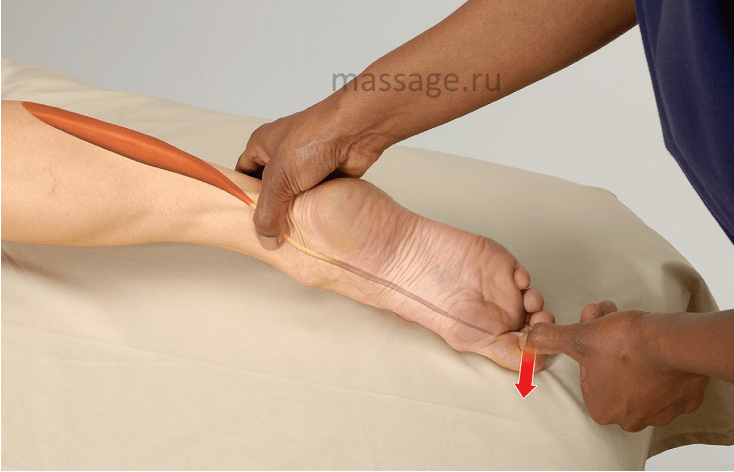
The client lies on his stomach
1. Standing at the client's feet, use your thumb to locate the medial malleolus.
2. In a smooth sliding motion, slide your thumb into the space between your ankle and Achilles tendon. (Caution: the tibial artery and nerve also pass through this area. Move your finger if the client feels tingling and numb, and if you feel a pulse.)
3. There are three tendons in this area. Palpate the tendon located most
is the tendon of the long flexor of the big toe.
4. Ask the client to bend their thumb to make sure you did everything right.
CLIENT EXERCISE: SEATED TOE STRETCH
1. Sit on the floor with your feet straight in front of you.
2. With your knees relaxed, bend at the waist and lean forward.
3. Take the big toe with your fingers.
4. Gently pull your thumb back towards your knee for 5-10 seconds, then release.
This exercise can be done with all toes.
- The long extensor of the thumb (lat. Musculus extensor hallucis longus) is the muscle of the lower leg of the anterior group.
Lies between the anterior tibial muscle (lat. M. tibialis anterior) and the long extensor of the fingers (lat. M. extensor digitorum). The upper two-thirds of the long extensor of the finger is covered by these muscles.
The muscle originates from the medial surface of the middle and lower thirds of the fibula and the interosseous membrane of the lower leg and, heading down, passes into a narrow long tendon, which passes under the lat along the middle canal. retinaculum mm. extensorum inferius to the big toe. It attaches to the distal phalanx. Part of its bundles fuses with the base of the proximal phalanx.
Related concepts
References in literature
long extensor thumb brushes. Along the radial edge of the forearm, it reaches the ulnar fold, then rising to the outer-posterior surface of the shoulder to the acromial process of the scapula and further to the seventh cervical vertebra. From this point, the meridian goes to the supraclavicular region, from where one of its branches goes deep into the body to the large intestine, and the second - along the neck, crossing the lower jaw in front of its angle. There he makes a turn, moving to the opposite side. In the nasolabial groove, it intersects with an identical meridian running along the other side of the body. There are 20 points along the meridian.
2. Meridian of the large intestine. Pair meridian. Refers to the Yang system. It starts from the nail bed of the index finger, runs along its radial edge, then goes between the first and second metacarpal bones and between the tendons of the short and long extensor thumb brushes. Along the radial edge of the forearm, it reaches the ulnar fold, then rising to the outer-posterior surface of the shoulder to the acromial process of the scapula and further to the seventh cervical vertebra. From this point, the meridian goes to the supraclavicular region, from where one of its branches goes deep into the body to the large intestine, and the second - along the neck, crossing the lower jaw in front of its angle. There he makes a turn, moving to the opposite side. In the nasolabial groove, it intersects with an identical meridian running along the other side of the body. There are 20 points along the meridian.
Related concepts (continued)
The pectoralis major muscle (Latin musculus pectoralis major) is a large superficial fan-shaped muscle located on the anterior surface of the chest. Under it is a triangular pectoralis minor muscle.
Round pronator (lat. Musculus pronator teres) is the thickest and shortest muscle of the surface layer. Two heads are distinguished in it: a large humeral head (lat. caput humerale), which starts from the medial epicondyle of the humerus, medial intermuscular septum of the shoulder and fascia of the forearm, and a smaller ulnar head (lat. caput ulnare), which lies under it and originates from medial edge of the tuberosity of the ulna. Both heads form an abdomen somewhat flattened from front to back, which ...
The quadriceps femoris muscle (lat. Musculus quadriceps femoris) - occupies the entire front and partly the lateral surface of the thigh. Consists of four heads.
The muscles of the upper limbs provide freedom and a wide variety of arm movements. The muscles of the upper limb are usually divided into the following groups: 1) muscles of the shoulder girdle; 2) muscles of the free upper limb - shoulder, forearm and hand.
The sartorius muscle (Latin musculus sartorius) is the muscle of the anterior thigh group. It is the longest muscle in the human body.
The latissimus dorsi muscle (Latin musculus latissimus dorsi) is a superficial muscle that occupies the entire lower back, the upper bundles in the initial part are covered by the trapezius muscle.
The small round muscle (lat. Musculus teres minor) is an oblong, somewhat rounded cord, the muscle bundles of which are parallel to each other.
The triceps muscle of the shoulder (triceps; lat. musculus triceps brachii) is the extensor muscle of the posterior group of the shoulder, occupies the entire back side of the shoulder, consists of three heads - long (caput longum), lateral (caput laterale) and medial (caput mediale).
The large round muscle (lat. Musculus teres major) is flat and elongated in shape. Throughout the posterior section it is covered by the latissimus dorsi muscle, in the outer section - by the long head of the triceps muscle of the shoulder, the deltoid muscle, and in the middle section - by the thin fascia.
The biceps muscle of the shoulder (biceps, lat. musculus biceps brachii) is a large muscle of the shoulder, clearly visible under the skin, due to which it is widely known even among people who are new to anatomy.
The coracobrachialis muscle (lat. Musculus coracobrachialis) is flat, covered throughout by the head of the biceps brachii. The muscle starts from the top of the coracoid process of the scapula and is attached below the middle of the medial surface of the humerus along the crest of the lesser tubercle.
The gluteus maximus muscle (lat. Gluteus maximus) is the largest muscle of the three gluteal muscles, which is closest to the surface. It makes up most of the shape and appearance of the buttocks.
The dorsal muscles are at the top of the foot (Fig. 10.39). The interosseous muscles, which occupy the space between the metatarsal bones, are also referred to as the dorsal muscles, since they are very easy to reach from the top of the foot. It is quite easy to treat the dorsal and interosseous muscles. Pain from trigger points in them is local in nature and is not transmitted to other places.
Extensors brevis and interosseus muscles
The extensor digitorum brevis lie under the extensor longus tendons at the top of the foot. Both extensor groups work together to lift your toes off the ground with every step you take.
Between the metatarsal bones there are two groups of interosseous muscles - dorsal and plantar. The third group of small muscles are worm-like - parallel to the metatarsal on the sole, but not located between them. The interosseous muscles allow the fingers to move from side to side and are involved in their flexion and extension. This mass of small muscles may seem like very little, but they play a big role in maintaining the balance of the body and adapting the feet to the ground. Their function is to restrain excess movements of the larger, but less sensitive muscles in the foot.
Symptoms
Pain from trigger points in the short extensors occurs immediately aroundthese muscles, which are located on top of the foot on its outer side (Fig. 1 0.39). In the figure, the extensor of four fingers consists of three heads of muscles adjacent to the four fingers. The extensor pollicis brevis is the only muscle that goes to the thumb.
Their common area of pain distribution coincides with the area of its distribution from  long extensor of the fingers, anterior tibial and third peroneal muscles. Sometimes you have to explore all of these muscles to find trigger points that cause pain. One woman would have suffered with legs for the rest of her life if she had not caught the eye of some new information.
long extensor of the fingers, anterior tibial and third peroneal muscles. Sometimes you have to explore all of these muscles to find trigger points that cause pain. One woman would have suffered with legs for the rest of her life if she had not caught the eye of some new information.
Pain from trigger points in the interosseous musclesfelt at the base of the toes, often extending to the tips of the toes (fig. 10.40). In some cases, the pain covers the entire back of the foot and goes up to the front of the lower leg (not shown). Trigger points in the interosseous muscles often cause cramps and swelling on the dorsum of the foot. A dull aching pain at the top of the foot can come from any dorsal plantar muscle. Trigger points in the first dorsal interosseous muscle can cause tingling in the thumb. In any of the zones, there is more numbness than pain.
The reasons
Walking, running, or climbing too frequently and vigorously can contribute to the formation of trigger points in any of the interosseous muscles or in any of the extensor muscles.  It is not uncommon for all of these muscles to have points, as they all depend on each other in this delicately balanced system of footwork. Be careful if the shoes are tight at the top of the foot. Tight shoes interfere with circulation and movement by creating problems with the interosseous muscles and extensor digitorum brevis. It's good to ditch high heels, because they cause the legs to roll towards the toes and all the muscles gather in front of the feet. On the other hand, if you are not used to walking barefoot, this can also negatively affect the muscles, causing them to strain unnecessarily.
It is not uncommon for all of these muscles to have points, as they all depend on each other in this delicately balanced system of footwork. Be careful if the shoes are tight at the top of the foot. Tight shoes interfere with circulation and movement by creating problems with the interosseous muscles and extensor digitorum brevis. It's good to ditch high heels, because they cause the legs to roll towards the toes and all the muscles gather in front of the feet. On the other hand, if you are not used to walking barefoot, this can also negatively affect the muscles, causing them to strain unnecessarily.
Treatment
Locate the short toe extensor muscles by their contraction as you lift your toes (Fig. 1 0.41). To massage the dorsal muscles, use only your fingertips or a weighted thumb.  These muscles are usually small and thin and do not require much pressure. To massage the interosseous muscles, dip the tips of two fingers or the thumb into the space between the metatarsal bones, above or below them (Fig. 10.42). Figures 10.43 and 10.44 show two other methods for interosseous massage. When the interosseous trigger points are active, it can cause a lot of pain and even trigger cramps if you push too hard. If, in an attempt to cope with a cramp in the arch of the foot, you begin to stretch it, cramps can occur in the interosseous muscles and in the short extensors at the top of the foot. If you are used to stretching your foot, pre-massage will reduce the risk.
These muscles are usually small and thin and do not require much pressure. To massage the interosseous muscles, dip the tips of two fingers or the thumb into the space between the metatarsal bones, above or below them (Fig. 10.42). Figures 10.43 and 10.44 show two other methods for interosseous massage. When the interosseous trigger points are active, it can cause a lot of pain and even trigger cramps if you push too hard. If, in an attempt to cope with a cramp in the arch of the foot, you begin to stretch it, cramps can occur in the interosseous muscles and in the short extensors at the top of the foot. If you are used to stretching your foot, pre-massage will reduce the risk.
The foot remains mobile due to the presence of various types of muscles in its structure, including the short extensor of the big toe. Short muscles are those muscles that do not go beyond the area of \u200b\u200bthe foot. The long ones are based at the ankle and attached to the foot. The most important function of these muscles is considered to be the flexion and extension of all fingers and the movement of the phalanges located on the feet.
Muscles localized in the toes are responsible for performing the correct movements of the bone levers in the ankle joint, and if they are damaged, the functioning of this entire department is disrupted. In the structure of the foot there are short and long muscles. There are also several flexors of the fingers: a short flexor of the foot of the little finger and other fingers. Foot mobility is provided by two extensor tendons.
short muscles
The extensor digitorum brevis is a muscle that looks like a wide, flat band that runs along the outside of the foot. It is attached to the heel bone, from where it moves to the fingers and there it is already transformed into three tendons. At the very top, they connect with other tendons, and then attach to the phalanges. The muscle is nourished with useful substances by the bloodstream, which moves along the tibial artery, and the supply of nerve sensitivity to these tissues is provided by the peroneal nerve.
long muscles
The long extensor of the big toes is attached to the tibia at one end and to the phalanges at the other. Its main function: flexes the thumb, unbends it. The extensor unites with the so-called square muscle and is divided into four tendons. All these tendons are attached to the four phalanges on the lower extremities, which allows you to bend and unbend the foot and move it in different directions. foot is located on the side of the lower leg on its outer side and is attached to the tibia. Further, it passes through the region of the lower leg and, penetrating the structure of the foot, is divided into five processes that are attached to the phalanges. This structure is responsible for the extension and flexion of the lower limb, its supination and is responsible for rotational movements.
Diseases and injuries of the long extensor are dangerous because they severely limit the mobility of the injured limb. For example, with tendinitis of the long extensor tendon, it becomes impossible to bend and straighten the fingers, gait is disturbed, such a condition without proper treatment can lead to disability.
Strengthening the feet with exercise therapy
The extensor of the big toe can be strengthened so that it is not damaged by excessive stress or various diseases. For this, various physical therapeutic exercises are performed. Such measures are considered an excellent prevention of leg pain.

There is such a term as the core of the legs, which means the totality of all the small muscles and tendons that stabilize the body during activity and movement. The function of these fabrics is to reduce and absorb the impact of walking while maintaining balance throughout the body. When these muscles are weakened, physical activity passes to the plantar fascia, in which pathological processes develop due to overstrain. The weakening of the ligamentous apparatus over time provokes a change in gait and becomes the root cause of pathologies in the knee and hip joints, and also causes disorders in the spine.
To strengthen the tendons and muscles of the foot, it is necessary to perform therapeutic exercises several times a week. The advantage of such physical education is that anyone can perform it at home. Below are some of the exercises that help strengthen the ligamentous apparatus on the legs.
- You should take a towel with your toes and stretch it around the room for several meters. Next, form a lump from this towel with your fingers. Grab the towel again and move it in the opposite direction. Repeat using the other lower limb.
- Scatter small objects on the floor - buttons, medium-sized balls and sit on a chair. Now try to collect these items of the feet in some kind of box. Repeat with the other leg.
- The first few times this exercise is carried out in a sitting position, then standing. You should put your foot on the floor, then pull your fingers towards you and at the same time you need to form an arc with your feet.
- Sit on the floor, legs extended forward in a straight position. Now you need to tighten the foot and stretch it in such a way as if you were standing on heels. Fix the position and try to slowly turn the foot towards you. Repeat several times.
A noticeable result can be noted after a few months of regular classes. The muscles are gradually strengthened, the arch of the foot rises. Blood circulation improves, the sensitivity of the foot increases, the stability of the whole organism is restored.
The muscles of the thumb of the hand recover from injury quite quickly - within one to two weeks. However, with sufficiently serious and / or chronic injuries of the thumb, damage to the structure of its tendons is often observed. Tendons are practically avascular structures, their blood supply is minimal. They recover from damage about six times slower than muscles. In addition, it is quite difficult to limit the mobility of the thumb during daily activities in order to allow damaged tendons to fully recover and prevent their re-injury.
That is why in the process of recovery after such injuries, the correct approach to therapy is extremely important. The sooner treatment begins, the faster recovery occurs. My first recommendation is not to start therapy immediately after an injury. You should wait at least 3-4 days to allow the scar tissue to fully form, and then you can apply techniques that include friction (friction massage). During the first few days after injury, you can resort to a light and shallow massage - this will help relieve pain and inflammation.
FRICTION APPLICATION
Based on my experience, I can confidently say that the most effective in the treatment of injuries of the tendons of the thumb demonstrate techniques that include friction. You can use your thumb or middle and index fingers to apply frictions. It is best to change your fingers frequently so as not to injure yourself.
Remember that pressure should only be applied in one direction. After you have worked the tendon with frictions in one direction, change the direction of the frictions to the opposite. This will help you avoid fatigue, ensure that all tendon fibers are evenly affected, and reduce the likelihood of discomfort for the client.
Work the tendon fibers in one direction for 4-5 minutes, rest a bit and start working in the other direction - in total you should spend about 8-10 minutes on this.
As the client's condition improves, the duration of therapy can be reduced. After applying the friction massage, you can gently stretch your thumb, hand and forearm.
DETERMINATION OF THE DAMAGED AREA AND THERAPY OF INJURIES OF THE TENDONS OF THE LONG AND SHORT EXTENDERS OF THE THUMB
Determining the damaged area of the tendon of the long or short extensor thumb is a very simple matter. Ask the client to extend the thumb so that the entire structure is in tension. Then apply frictional strokes of low or medium intensity across the fibers of the tendon of the short or long extensor of the thumb (depending on the nature and location of the injury). Do this at various points along the tendon to pinpoint the location of the damaged fibers. Since pain in these injuries does not radiate to nearby structures, the location of damaged fibers can be easily determined by the localization of pain sensations.
Once you have determined which part of the tendon is damaged, ask the client to relax the finger and then proceed with the friction massage. Each stroke should completely cross the damaged area.
This approach is applicable in the treatment of any tendon injury. Remember that it is necessary to determine the location of the damaged area quickly enough - with tendon injuries, prolonged stress
contraindicated.
DETERMINATION OF THE DAMAGED AREA AND THERAPY OF INJURIES OF THE SHORT AND LONG FLEXOR TENDONS OF THE THUMB
The tendons of the long and short flexors of the thumb are not so easily amenable to therapy, and it is also quite difficult to determine the damaged area. We will focus on the flexor hallucis longus tendon, as this tendon is the most commonly injured.
With one hand, hold the pad of the thumb as shown in the picture and ask the client to try to bend the finger. With the other hand, palpate the damaged tendon located in the middle part of the thumb eminence (closer to the index finger) along its length until you find the localization of pain. The client must hold the finger in tension for a while to give you the opportunity to find the damaged area. Once you have identified the damaged part of the tendon, the client can relax the finger. Perform friction at an angle of 90 degrees to the tendon fibers for 4-5 minutes, rest and repeat this action. The total duration of therapy should be 8-10 minutes, excluding one or two breaks.
DETERMINATION OF THE DAMAGED AREA AND THERAPY OF INJURIES OF THE TENDONS OF THE LONG AND SHORT MUSCLE THAT REDUCE THE THUMB
With injuries of the muscles that remove the thumb, the tendon of the long muscle that removes the thumb of the hand, located immediately behind the tendon of the short extensor thumb, most often suffers. That is why we will focus on this particular tendon.
Have the client abduct the thumb to locate the tendon. It is located slightly anterior and posterior to the extensor pollicis brevis tendon. Have the client move their thumb from side to side so that you can separate the abductor pollicis longus tendon and the extensor pollicis brevis tendon. They are located very close, therefore, in order to find the tendon of the abductor muscle, a little effort should be applied. Once you have located the tendon, palpate it to pinpoint the damaged area or areas. The main symptom of damage is local pain. Once you have located the damaged areas, ask the client to relax the thumb and proceed with therapy.
DETERMINATION OF THE DAMAGED AREA AND THERAPY OF INJURIES OF THE TENDONS OF THE ADDUCTIVE THUMB MUSCLE
Place your thumb on the medial interphalangeal joint of the thumb, and ask the client to bring the finger to the other fingers.
Use your thumb or other fingers of the other hand to palpate distally and proximal to the interphalangeal joint. Palpate the tendon fibers to locate areas of pain, then ask the client to relax the finger and get to work. As the client's condition improves, include strengthening exercises that the client can do at home. If these exercises cause pain or discomfort, then it is not time to move on to this phase of therapy. Wait at least another week. Start with simple isometric exercises like the ones I'll describe below.
EXERCISES FOR THE CLIENT
I will describe these exercises using only one hand as an example. Have the client place the pad of their index finger on the thumbnail and then try to straighten the thumb, holding it in tension for a few seconds. Then ask the client to place the top of the index finger under the ball of the thumb and then try to bend the thumb while holding it in tension for a few seconds. After that, the client should place the tip of the index finger on the medial part of the thumb between its tip and the first joint, and then try to bring the thumb to the other fingers. Then the client should place the tip of the index finger on the side of the thumb and try to move it to the side.
These exercises allow you to train your thumb in four planes without using any additional sports accessories. I recommend repeating these isometric exercises for 5 sets 4-5 times throughout the day. I believe that this is the most affordable and effective way to strengthen the muscles and tendons of the thumb.
Dr. Ben E. Benjamin
Source: www.massage.ru
Anatomy
The long extensor of the fingers refers to the muscles of the lower leg, or rather, to its anterior group. It is located outside of the anterior tibial muscle. The muscle goes down, turning into a narrow tendon, which is amazingly strong. Further, it diverges into 4 beams: each is designed for a separate finger. It is attached at the level of the proximal phalanx. At the attachment point, the beam diverges into 3 small parts, which make it possible to set in motion any part of the foot.
The mobility of the thumb is carried out by the work of several muscles at the same time. This complex structure is necessary, as it is he who helps to maintain balance and the ability to walk upright. The long flexor of the big toe is a muscle that belongs to the posterior group of the lower leg. Its growth begins in the region of the lower 2/3 of the fibula. It goes down the limb to the sole and turns into a tendon. On the foot, it grows a little into the tendon responsible for the movements of the remaining fingers. So it turns out that the movements of all phalanges depend to one degree or another on his work. It is fixed on the nail phalanx.
Muscles responsible for flexion and extension of the fingers
The extensor muscles in the lower extremities are appropriately named and do heavy work on a daily basis during movement. These include:
- tibialis anterior,
- long extensor,
- thumb extensor.
The calf extensors are very strong and important for the ability to walk straight.
bending
The long flexor makes it possible during movement (when a person is walking or running) to push off the floor in the right way. He also participates in the supination of the foot - the ability to stand on the toe and maintain balance.
The long flexor of the thumb is named for its functions: it helps to bend it, and can also affect the entire metatarsus due to the features of its structure. Like other muscles of the lower leg, it is involved in the work of the foot, helping it to bend, as well as adducting and supinating. Also, the presence of this tendon makes the longitudinal arch of the foot stronger.
Extension
The long extensor is included in the group of muscles of the lower leg, located in front, closer to the inside. In addition to its direct purpose, this tendon extends the foot. To do this, it works together with the 3rd peroneal muscle. In the case of rigid fixation of the foot, it will bring the lower leg closer to it.
The long extensor of the thumb is responsible for the ability to straighten the big toe, and also sets the foot in motion, raising its front edge.
Muscle performance tests
The calf extensors can lose their strength due to a number of reasons. You can check its condition and performance using simple tests that the doctor conducts during the examination:
- With one hand, you need to hold the metatarsus in the usual position, and with the other, gently but firmly bend your toes. A person should strive to straighten them. If he succeeds, the highest mark is 4 or 5.
- The person lies on his back, a soft roller is placed under his knees. The metatarsus is held by force. At the same time, he should try to straighten his fingers. If he succeeds, the highest mark is 3.
- The position is the same. The doctor feels the tendon, while the person should try to straighten his fingers. If he succeeds, the highest mark is 1.
In a normal state, a person receives 5 points. The strength may decrease if the tissues do not receive sufficient nutrition, or if innervation has occurred.
Causes of muscle dysfunction
The foot extensors can lose strength or suffer other damaging effects for a number of reasons:
- atrophy with age due to disruption of tissue nutrition,
- pathologies in the work of the endocrine system,
- connective tissue diseases,
- fermentopathy,
- polyneuritis,
- complications after injury
- too much physical activity.
The main cause of the lesion is tendonitis. This is an inflammatory disease of the tendons that can also affect nearby muscle tissue. Dystrophic destruction can become chronic, which is very dangerous and almost incurable.
Also, pain in the foot can occur due to the deposition of salts and the formation of growths on the bone tissue. The reason for this may be the use of certain drugs, etc.
Diagnostics
The extensor hallucis longus or the entire metatarsus may be damaged. On examination, the doctor notes "spanking" when walking or dragging. The doctor performs palpation, as well as a series of tests that help assess the nature of the damage. If muscles have been damaged, weakness and soreness may occur when exercising with or without resistance. If there is weakness of the entire metatarsus, including the little finger, compression of the nerve is possible.